My anecdotal experience and studies have shown me thIs:-
In cooking at oven temps this is a desirable and flavoursome reaction at some speed.

My anecdotal experience and studies have shown me thIs:-
In cooking at oven temps this is a desirable and flavoursome reaction at some speed.

2004; 97: 229-35
productive over the long-term.
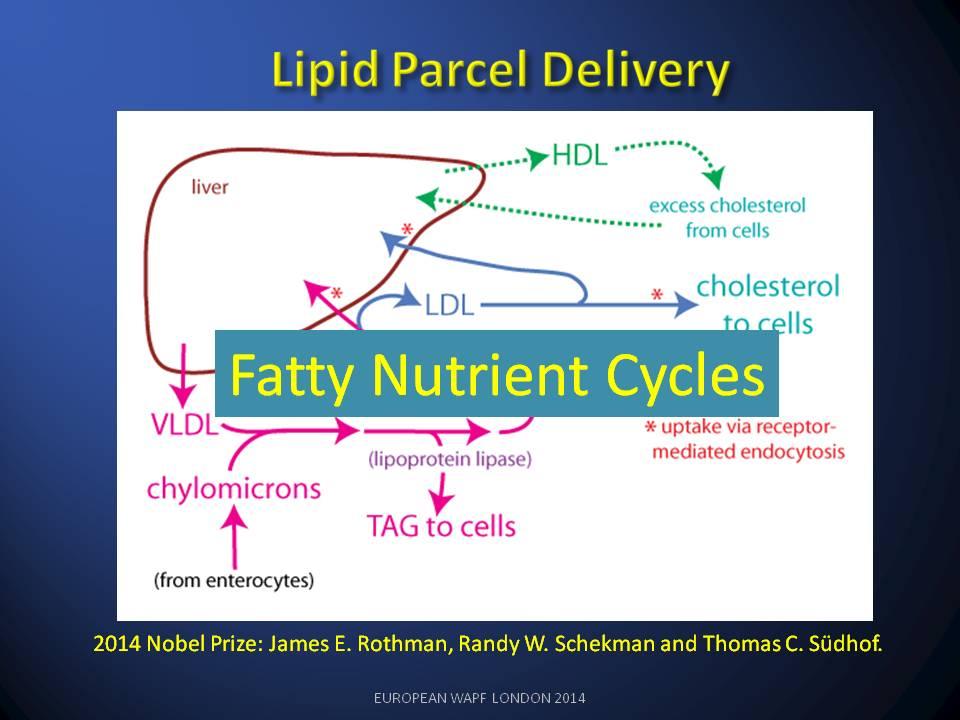
The 2013 Nobel Prize for Medicine raised expectations of a parallel discussion of extra-cellular lipid circulation in The Lipid Cycle. A better understanding of the health problems caused by disruption to The Lipid Cycle has been blocked for over 40 years by incorrect use of the chemical term ‘cholesterol’ as an inaccurate surrogate when referring to Lipid profiles. This singular error has caused decades of misunderstanding and inappropriate treatments in medicine.

Understand this means it should have better been called ‘Bad-LDL’.

The HDL lipid class operate on the return side of the lipid cycle and is depleted when LDL is damaged.

/* Style Definitions */
table.MsoNormalTable
{mso-style-name:”Table Normal”;
mso-tstyle-rowband-size:0;
mso-tstyle-colband-size:0;
mso-style-noshow:yes;
mso-style-priority:99;
mso-style-qformat:yes;
mso-style-parent:””;
mso-padding-alt:0cm 5.4pt 0cm 5.4pt;
mso-para-margin-top:0cm;
mso-para-margin-right:0cm;
mso-para-margin-bottom:10.0pt;
mso-para-margin-left:0cm;
line-height:115%;
mso-pagination:widow-orphan;
font-size:11.0pt;
font-family:”Calibri”,”sans-serif”;
mso-ascii-font-family:Calibri;
mso-ascii-theme-font:minor-latin;
mso-fareast-font-family:”Times New Roman”;
mso-fareast-theme-font:minor-fareast;
mso-hansi-font-family:Calibri;
mso-hansi-theme-font:minor-latin;}
Thank you Dr Verner Wheelock for the extensive critique of the reports . The Cochrane reports analysis was heroic and well structured. We had a huge debate about them at the time on THINCS (www.thincs.org).
For my part I shy away from statistical analysis which doesn’t include ‘All Cause Mortality’ figures. The reason being that failure to look at all the non-cardio deaths and drop-outs from trials cleans and amplifies the apparent benefits of Statins. This means we can never know the Numbers Needed to Harm NNH side of the medication.
My first ever review paper (G Wainwright et al., 2009) looking at the clinical impact of cholesterol lowering in all non-cardiovascular organs, was seminal in that it pointed up a fundamental flaw in the whole statin concept i.e. Cholesterol is vital and inhibiting its production is destined to create a wide and varied set of Adverse Events in statin users in the longer term. That is why ‘all cause mortality’ data is not made available (caveat emptor).
In our second review paper(Seneff et al., 2011) we became aware of the fact that LDL/HDL ratios were associated with LDL consumption by organs and not production by the liver. The whole LDL argument had been inverted. If LDL is damaged by glycation, LDL goes up and HDL falls. The liver’s glycated-LDL is unused and the corresponding HDL return to the liver does not happen.
How such a fundamental part of the lipid nutrition cycle could be missed is hard to understand. Obsession with statins and statin finance has done immense harm to cardio-medicine and I believe we are seeing the start of a major NICE scandal as the BMA object to the guidance.
From today my name’s on the blog (I keep typing Blob!), I’ve taken over from Liz W.
Something to do on a rainy day.
I don’t mind the rain. Sometimes you need the rain to hide your tears.
The treatment and placebo groups’ mortality lines should be independent: a trend in one should have no consequential influence on the other. However:
- All 4 lines are essentially identical for 1.6 years.
- Then there is a departure — by both lines at the same time.
The fact that both lines — treatment and placebo — depart at the same time is important. Why should the treatment suddenly become beneficial at exactly the same time as non-treatment becomes detrimental?
The average line of both treatment and non-treatment groups follows a ‘natural’ mortality curve; any natural survival curve would have its slope increasing downward. (i.e. becoming more negative.)
Both treatment and placebo lines follow this natural curve for 1.6 years. Then both diverge. The placebo group shows this slope change increasing (negative) at a faster rate than all other lines. But, surely, it should follow the natural mortality curve. Why doesn’t it?
The slope of the treatment group is nearly constant from 1.8 years onward. It’s not a curve at all, but an almost straight line — and it shouldn’t be. What it says is that old people die at the same rate as younger ones. And life isn’t like that.
Is this evidence that the data of the 4S trial were not handled in an honest manner? Were deaths occurring in the treatment group assigned to the placebo group? Is this why the two curves, which should be independent, are apparently related? Or is there a mistake somewhere? Is there an error in logic?
The inability of current recommendations to control the epidemic of diabetes, the specific failure of the prevailing low-fat diets to improve obesity, cardiovascular risk or general health and the persistent reports of some serious side effects of commonly prescribed diabetic medications, in combination with the continued success of low-carbohydrate diets in the treatment of diabetes and metabolic syndrome without significant side effects, point to the need for a reappraisal of dietary guidelines.
•They present major evidence for low-carbohydrate diets as first approach for diabetes.•Such diets reliably reduce high blood glucose, the most salient feature of diabetes.•Benefits do not require weight loss although nothing is better for weight reduction.•Carbohydrate-restricted diets reduce or eliminate medication.
•There are no side effects comparable to those seen in intensive treatment with drugs.
Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ, Westman EC, Accurso A, Frasetto L, McFarlane S, Nielsen JV, Krarup T, Gower BA, Saslow L, Roth KS, Vernon MC, Volek JS, Wilshire GB, Dahlqvist A, Sundberg R, Childers A, Morrison K, Manninen AH, Dashti H, Wood RJ, Wortman J, Worm N, Dietary Carbohydrate restriction as the first approach in diabetes management. Critical review and evidence base, Nutrition (2014), doi: 10.1016/j.nut.2014.06.011.
You can’t get funding very easily for lifestyle trials because there is no profit to be made. Or is there? Medical Insurance and NHS costs would be reduced dramatically – so there is a cost reduction motive for funding!
Dietary Carbohydrate restriction as the first approach in diabetes management


