We know that all cells (all tissues) cease their exocytosis and endocytosis activity, if the membrane cholesterol content drops by
around 10%. This is easily achieved on statin therapy. Everything slows down.
In the case of bone remodelling both osteoclasts (cutters) and osteoblasts (builders) will reduce their repair activity in bone remodelling.
Calcium loss from bones will be reduced but micro-fracture repairs will not be repaired on statin therapy. Bone density is maintained on statin therapy but the developing micro-fractures weaken the skeleton.
It’s all about what is measured and how long you follow through.
Statin trials can be designed to prove both benefit and detriment to bones.
This is why experimental osteoporosis treatment by statins to maintain bone density ultimately gives way to increased fracture risk.
Two competing bone remodelling processes are failing and conflicting measures can be used to conflict statin safety.

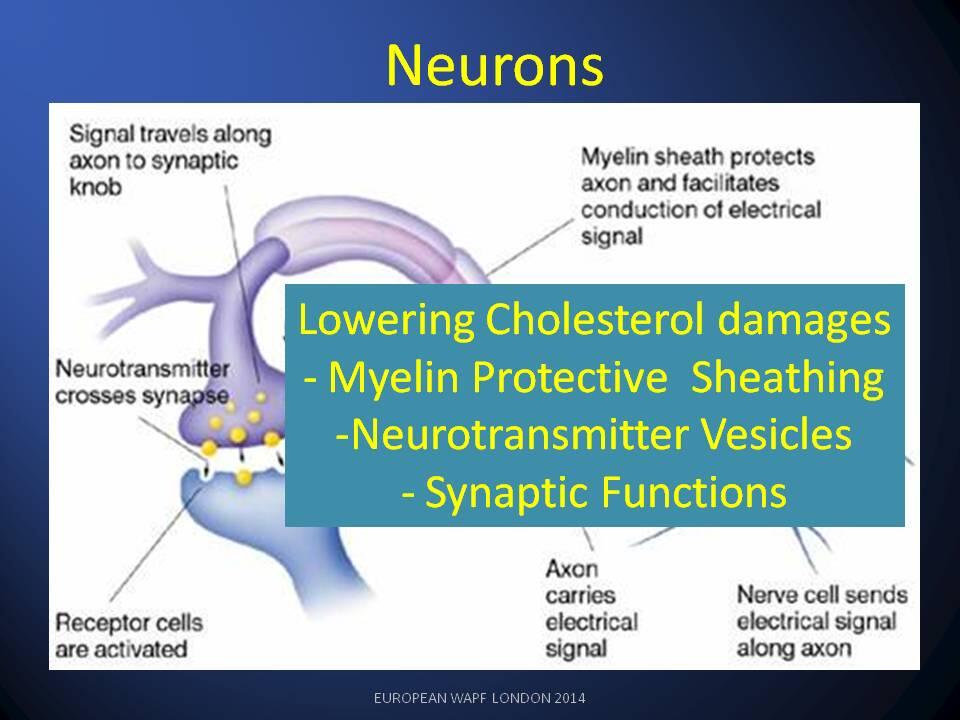
You will find this pattern repeats in damage and repair of myelin in MS studies.
To summarise: Short-term gain- long-term pain on statins
Dr Luca Mascitelli and myself went into this in our review paper 2009 at http://bit.ly/Ob9wKM